The fight against the epidemic has made the improvement of medical electronic technology a focus of attention. Let’s take a look at this article. What do you think?
[Copy link]
Fully integrated optical modules enable higher specification performance
Photoplethysmography (PPG) is a common technique for measuring blood oxygen saturation (SPO2) levels. A light transmitter is used to emit light into the body, and a light receiver is used to measure the amount of light that is reflected or not absorbed. Based on the ratio of the two wavelengths, the amount of oxygenated hemoglobin can be measured. Similar techniques are also used to measure heart rate (in conjunction with optical techniques) or heart rate variability.
All of these systems require the use of one or more optical transmitters (which need to be controlled), and a photodetector to measure the amount of light received. This received signal ultimately needs to be amplified, conditioned, and digitized. This optical system may sound simple enough; however, without any knowledge of optics, it is easy to retrieve an optical signal that has nothing to do with the signal the user is looking for.
To help companies achieve their optical goals, we have introduced a new fully integrated optical module. This module has been tested and compared to a mature discrete optical system with impressive results. We will detail the results and methodology used in this testing.
PPG Measurement Theory and Introduction
With the increased focus on family health, wellness and prevention, a new market has formed around smart devices that track multiple vital sign parameters. First there were chest straps that used biopotential technology to monitor heart rate, but in the last 5 to 8 years the market has generally moved to optical systems that use photoplethysmography (PPG). One of the great advantages of this technology is that we can measure at one point on the body, whereas biopotential systems require a minimum of two electrodes to measure the heart. This is not very convenient for the user, and as a result, interest in optical heart rate monitoring (HRM) and heart rate variability (HRV) monitoring has increased dramatically.
Before designing such a system, several questions need to be answered. What is the end application? Where in the human body do you want to measure? How much time do you have to develop the system? Depending on the answers to these questions, the designer may take different design paths.
There are two different principles for measuring PPG. You can either pass light through a body part, such as a finger or earlobe, and measure the amount of light received or not absorbed on the opposite side; or you can send light on the same side of the body and measure the amount of light reflected. Measuring the amount of light that passes through the body gives about 40 dB to 60 dB more signal than a reflective system; however, with a reflective system you can freely choose where to place the sensor.

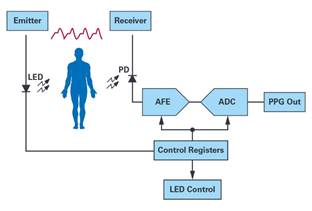
Figure 1. Typical block diagram of an optical HRM/HRV system.
Since most users value sensor comfort more than performance, the reflection measurement method is more popular. Therefore, this article only introduces the reflection measurement technology.
During a heartbeat, blood flow in the cardiac system changes, causing the received reflected light to scatter. The wavelength of the light source used to measure optical HRM/HRV depends not only on the measurement point on the body, but also on the relative perfusion level, as well as the temperature and color tone of the tissue. Typically, for wrist-worn devices, the artery is not located at the top of the wrist, and you need to detect the pulsating component from the veins and capillaries below the surface of the skin. In this case, green light gives the best results. In locations with sufficient blood flow, such as the upper arm, temple, or ear canal, it may be more effective to use red light or infrared light, which can penetrate deeper into the tissue and give a stronger received signal.
ADPD188 Is the game changing?
When weighing trade-offs, such as sensor location and LED wavelength, you need to choose the most appropriate optical solution. There are many choices for analog front ends, either discrete or fully integrated, and a large selection of photodetectors and LEDs. The key is to place the transmitter and receiver in a way that maximizes the amount of received signal per milliamp of transmitted current. This is called the current transfer ratio and is usually expressed in nA/mA. In optical systems, the modulation index is also important, which is the amount of AC signal relative to the optical DC bias. When increasing the distance between the light sensor and the LED, the modulation index increases. There is a sweet spot between the photodetector and the LED, which also depends on the LED wavelength. In a poorly designed mechanical system, the LED light can reach the light sensor directly without penetrating the human tissue. This causes a DC bias that adversely affects the modulation index. It manifests as optical crosstalk, also known as internal light pollution (ILP).
To minimize the design effort and reduce time to market, especially for companies with little optical knowledge, Analog Devices has built a fully integrated optical subsystem for reflectance measurements. The ADPD188GG contains all the components needed to perform optical measurements. Figure 2 shows a photo of this module.
Figure 2. ADPD188GG optical subsystem
The ADPD188GG is a completely new design of optical module with different dimensions compared to the previous generation modules. It has an almost square shape with dimensions of 3.98 mm x 5.0 mm and an overall thickness of 0.9 mm. The most modified part is the photodetector, which is rotated 90° compared to the previous generation. This position of the sensor relative to the LED allows for higher sensitivity. The light sensor itself is available in 0.4 mm2 and 0.8 mm2. This provides flexibility to increase the overall photodiode surface for higher sensitivity or to use a smaller detector to prevent the sensor from saturating. The photodiode is placed on top of the analog front end. ADI is using the standalone ADPD1080AFE. It has 4 input channels, each designed around a transimpedance amplifier with selectable gain (25k, 50k, 100k, and 200k), an ambient light rejection block, and a 14-bit SAR ADC. The ambient light rejection is done in the analog domain and offers better performance than other solutions available on the market. Finally, the two green LEDs are controlled by an integrated current source capable of driving up to 370 mA with 1 μs narrow pulses to reduce the overall average current. The package design makes it difficult for the emitted LED light to reach the light sensor without penetrating human tissue. This prevents optical crosstalk and provides the user with the best modulation index, even if the sensor is placed under a glass or plastic window. This feature is very useful when designing optical reflective systems. For applications where emission measurements are more appropriate, the ADPD188GG can bypass the internal LEDs and work with externally connected LEDs.
Comparison with mature solutions
Before starting a new optical design, it is important to determine the target market and the specifications required for the final product. Generally speaking, optical systems with medical-grade performance will have higher specifications than those for devices used in the sports and healthcare markets.
The ADPD107 is an analog optical front end for discrete optical systems. It is considered a benchmark product among the optical front ends on the market and is widely used in many medical products due to its excellent performance. DataSenseLabs Ltd. has extensive experience with the ADPD107. However, since fully integrated optical modules have certain advantages in certain use cases, DataSenseLabs Ltd. started to study these modules and conduct a comparative analysis to compare the performance between the ADPD107 and the ADPD188GG integrated optical module. Next, we will describe the test setup, configuration, and test results in detail.
Test Setup and Data Collection
For optical comparison, raw PPG readings from the ADPD188GG and ADPD107 were recorded simultaneously over a 2-minute period. The ADPD188GG was set up using a standard evaluation board, while the ADPD107 was part of an optical system inside a wearable demonstration platform (EVAL-HCRWATCH). Both systems were controlled by the ADI user interface application, wavetool software.
For testing purposes, the configuration settings were optimized to achieve the highest signal quality. The AFE configuration was retained, including keeping the LED pulses, timing, and transimpedance gain within a specific range to keep the power consumption of both systems the same for a fair comparison (see Table 1).
Table 1. Optical module comparison between ADPD188GG and reference product ADPD107
Table 1 shows the ADPD188GG LED current, which is up to 2 times the LED current in the ADPD107 setup. The reason is that the photodiode surface of the integrated solution is smaller than that of the discrete solution, and this must be compensated. Using two LEDs powered by a 3 V supply increases the overall power consumption by 156 μW, which is almost negligible compared to the overall power consumption. We sampled the ADC at 100 Hz, which is very common in wearable systems. In addition, we measured at a sampling rate of 500 Hz, which is common in systems with clinical performance.
The data recording environment is the same as that of a regular smartwatch or fitness tracker, except that the optical sensor is located above the wrist. Since the microcirculatory and vasoconstriction properties of the subcutaneous layer of the dominant and non-dominant hands are slightly different, the two optical systems repeatedly record data from both wrists. The data sets collected from the left and right wrists are then carefully analyzed and compared to avoid any impact on signal quality due to placement. The PPG data set comes from 11 different users (subjects) who were all seated and exposed to the same ambient light density conditions.
Data analysis and statistics
A comparative approach is important because signal quality verification means more than just hard science signal processing, data analysis and statistics, it also involves analyzing the market and end-user expectations. To succeed in the wearable market, you need to have well-defined use cases and a clear idea of what results you want to achieve with your optical signals.
Optical heart rate monitors are closely associated with fitness tracking and health monitoring applications, but there are also many use cases where optical technology can be used in medical-grade systems. In fitness, health informatics or medical-related use cases, the accuracy of the peak detection algorithm depends mainly on the raw data quality, which is related to the local maxima of the PPG signal. Accurate peak detection is not only a principle for implementing heart rate or HRV measurements, but is also extremely important when implementing PPG-based blood pressure estimation. Therefore, if the final extracted and calculated PPG signal is to be used to support health-related applications, designers must choose a sensor platform that provides the best physical signal quality. The comparative measurement configuration and data analysis are designed and implemented based on János Pálhalmi's biosignal measurement patent (pending ID: P1900302). 1
Final Result
To support the peak detection algorithm, baseline fluctuations in the PPG raw data can be easily extracted and filtered. At the same time, as mentioned above, to extract the target result, the peak needs to have high signal quality at the raw data level. Therefore, this article focuses on the comparative analysis of the main frequency bands, targeting the peak of the PPG signal measured by the classic product ADPD107 and the newly integrated ADPD188GG optical module. The main part of the signal is unchanged, but the very slow baseline fluctuations (
Figure 3. Individual PPG waveforms (±125 data points around the local maximum) are extracted and overlaid on each other for comparison (blue dotted lines).
The overall average of the waveform is shown in red. The figure above shows the ADPD188GG and ADPD107 discrete solutions.
Similarities between the recorded PPG signals.
Wavelet coherence and correlation comparisons were calculated to compare the stability between the two signals in the most dominant frequency range. Figure 3 shows that the pattern of results for both PPG systems is almost identical on the individual waveforms and their averages.
To continue the comparison at a deeper data level, we used two different correlation-based approaches. Correlation coefficients and P values (R, P) were calculated between each of the upcoming PPG waveforms. Another signal difference could also be tested by comparing each individual PPG waveform to the mean.
Based on the comprehensive correlation tests, we can conclude that it is unlikely that there will be large differences between the two compared PPG systems, either at the level of individual waveforms or at the level of comparison of individual waveforms to the average.
The wavelet method is very sensitive to differences within a specific frequency band. Therefore, we calculated the wavelet coherence function to compare the two PPG signals. Based on the analysis results of all 11 subjects, there was no significant difference between the two signals in the frequency domain or phase domain (see Figure 4).
Figure 4. The amplitude square wave coherence between the ensemble averages of two compared PPG signals is represented by color intensity plots in the time and frequency domains. The direction of the arrows is proportional to the phase difference between the signals. A horizontal signal pointing to the right indicates that there is no phase difference between the signals.
When developing new products, it may also be useful to look at specific frequency bands that can be extracted from a given signal and used to optimize product specifications.
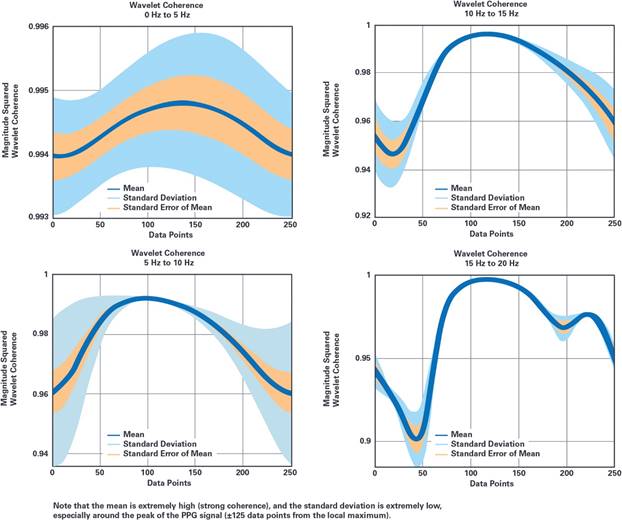
In this test, the basic statistical properties of the amplitude square wave coherence between the two PPG systems being compared were analyzed over all relevant frequency ranges, as shown in Figure 5. The entire spectrum was divided into six specific frequency ranges to analyze the similarities and differences between the signals.
For all 11 subjects, the coherence values were higher than 0.95 in all frequency bands around the PPG signal peak, indicating that the similarity between the benchmark product and the newly integrated ADPD188GG is very high.
Figure 5. Descriptive statistics of the amplitude square wavelet coherence values are shown over the 4 relevant frequency ranges (0 Hz to 20 Hz). 1
in conclusion
ADPD188GG is a fully integrated optical module from Analog Devices that measures heart rate, heart rate variability, and oxygen saturation, and monitors continuous blood pressure estimation. Since the module integrates both optics and electronics in a tiny package, it can help designers and companies with little optical knowledge to shorten the overall design cycle. The module is optimized for applications using a reflective measurement method at a wavelength of 525 nm; however, external LEDs can also be used to measure at different wavelengths or based on the emission principle. We have proven that an integrated system does not prevent us from meeting the specifications required for each use case in an out-of-hospital system or a clinical system.
| 








 提升卡
提升卡 变色卡
变色卡 千斤顶
千斤顶



 京公网安备 11010802033920号
京公网安备 11010802033920号
